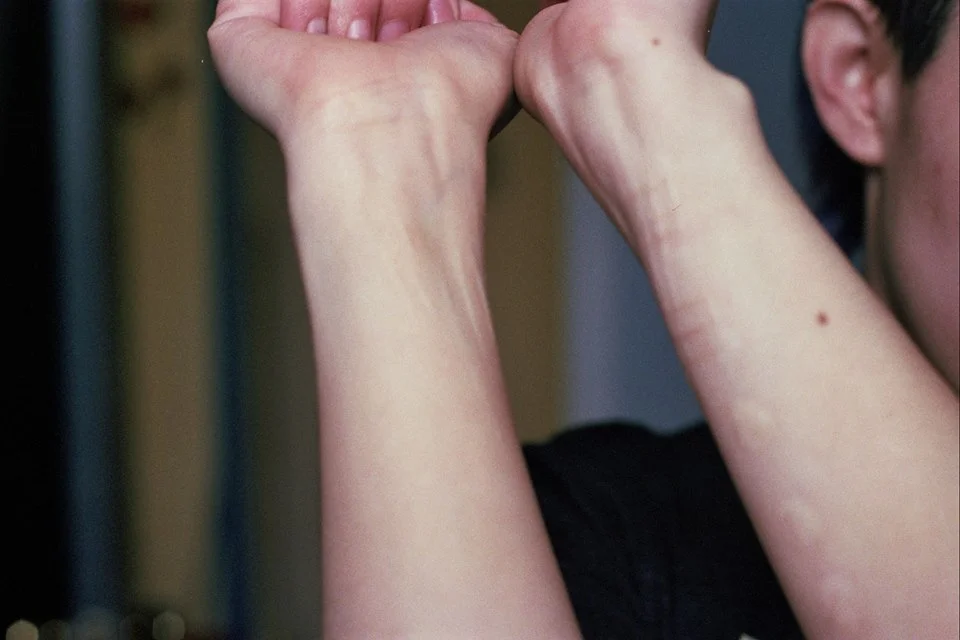
Photo by Eli Sleepless
Mental health is white.
The phrase “mental health” often fails to capture our experiences as people of color. What I mean is that white therapists, white researchers, white patients are the only visible people in mental health systems. The picture of depression is an overworked white man. When we think of anxiety, we think of white college students or a new (white) parent struggling to adapt. Even the idea of queer mental health centers whiteness, rarely considering other intersections.
White people get therapy, and people of color get left out.
I already covered three ways that mental health is different for people of color. In that article, I emphasized that trauma is often woven into the fabric of our lives, especially if we consider the emerging research on how ancestral trauma might impact a person’s genes today. Yet when people of color seek support, these cultural factors aren’t considered by the people who claim to offer help.
One of my favorite quotes on survival at the intersections of oppression is from Radical Dharma: Talking Race, Love & Liberation. Rev. angel Kyodo williams writes: “Our healing cannot wait until the structures acquiesce, are dismantled, or come undone.”
It’s a powerful truth that motivates me to keep going in my own search for healing. However, it reminds me that unfortunately mending our wounds often means finding support within the systems that harm us. To have any chance at succeeding, we need to continue naming the barriers that we butt against and hope to overcome.
1) There’s less support available for people of color within our own communities and the mental health system.
This has multiple repercussions, including learned helplessness to the point we stop asking for support and pressure ourselves to be “strong enough” to solve everything alone.
It’s important here to note that POC communities aren’t any more ableist or anti-mental illness than non-POC communities. However, people of color with chronic mental health issues are more oppressed, and part of that oppression is denial of our pain.
Since there is a general denial of the struggles of POC within the mental health system itself – including underdiagnosis, disbelief in our trauma, and minimizing our concerns when we finally do voice them – we can all-too-easily act in denial towards one another. Society teaches us to turn away from other people’s pain, especially that of marginalized people. We are then not only underdiagnosed and underserved by the mental health system, but also unable to access the needed care from our loved ones.
In multiple peer support spaces, I’ve witnessed and been swept up in the pressure for POC to perform emotional labor without getting that support back from the group. It can feel like, without giving and giving more, we won’t be seen at all. But even when we are seen, it’s in stereotypical roles – roles that don’t leave space for us to be struggling with our mental health or the racism of our peers.
2) Mental health and racism are never separate, even when the therapist says otherwise.
This connection shows itself in a lot of subtle ways like how years of racist, anti-Black, and/or colorist remarks contribute to depression. The oppressive bullshit can be so prevalent it’s hard to map out how all those microaggressions can lead to internalizing fucked up (false) beliefs about ourselves. Or it can be hard to help someone else see how racial stereotypes, like docile Asians or strong Black women, can change the way we experience and express challenging emotions like anxiety and anger.
Like many people of color, I’m still impacted by racist bullying from way back in elementary school. I remember being 9 years old sitting at my school desk trimming my arm hair with scissors because I thought being hairy would repel people. And even though I stopped bothering with my arm hair, the same obsession morphed into various things like showering just to shave; knowing my body could grow so much hair, even without allowing it to be visible, felt dirty.
Not only are mental health and racism deeply intertwined, but that connection is too often overlooked or denied. A couple years ago I read this article, “OCD: #whitepeopleproblems?” in which a white person with OCD wrote about how people of color can be obsessive-compulsive too. Like oh, wow, can you believe it! In doing so, she centered herself and incorrectly explained it as two separate struggles: surviving racism and managing OCD. She erased the overlap.
Intersectional mental health isn’t neat and tidy, with one problem over here and the other over there, and the messiness is what we need support to work through. Yet most white mental health professionals will deny this messy complication and try to make people of color fit into a narrow definitions of anxiety, depression, or another disorder. That impacts not only our care in the mental health system, but also how we see ourselves.
3) We’re left out of research, especially drug trials, and then blamed when treatment methods don’t work for us.
Almost all drug trials in the United States focus on white people – and often white men, specifically. When clinicians fail to recognize that other communities may react in different ways to commonly prescribed medication, the rest of us are forced into a limited model of “care” created for people who are facing different challenges. Even if the clinical label being treated is the same, individual experiences vary a lot, especially for those of us with oppressed identities.
There’s a label for people who don’t fit into common models of mental health care: “treatment-resistant.” This framing places blame on the individual and not the system. The resistance to treatment isn’t a failure to comply with their medication regimen, which many falsely believe. It refers to a physiological resistance when someone reacts to medication in unexpected ways. Just because a prescription works for one person with depression doesn’t mean it works for every person with depression, but those of us who are “treatment-resistant” are deviant. And that makes us the problem for being unwell. Only those who are “working hard” on healing get well, at least according to the system.
I’ve been treatment-resistant since I was a teenager because I experience atypical reactions to psych meds. For example, the tranquilizer Seroquel makes me manic, whereas the mood stabilizer Depakote made me the most monotonously depressed I’ve ever been in my life. When that isn’t happening, I face severe side effects that knock me out one way or another.
I know debilitating side effects are common, but when we’re surviving without enough support, it can be impractical and even inhumane to expect disabled people to wait out intense side effects on top of managing the symptoms being treated. We need reliable housing, food, and health care at the very least to get through that process. Many of us don’t have that.
It’s only recently, at least a decade later, that I finally got clarity about why I react to meds in surprising ways. A social worker friend Shivani Seth told me that they came across research showing that South Asians commonly have negative reactions to psychiatric prescriptions. But we aren’t being studied in drug trials, so there’s little record of this, and most mental health professionals have no fucking clue.
Once again, people of color just aren’t being considered, not even to ensure the safety and efficacy of mental health treatment.
* * *
This is far from an exhaustive list of ways that mental health is different for people of color, especially when we’re at intersections of oppression due to disabilities and other identities. If you have something to add about your own experiences with mental health as a trans and/or queer person of color, consider contributing to Rest for Resistance. We publish all genres as long as it’s about self-care, survival, or that elusive emotional wellbeing. E-mail qtpocmentalhealth@gmail.com with your ideas. (No response guaranteed because of limited capacity.)
And if you want to help change the image of mental health so that it includes all people and diverse concerns, please donate. We run entirely on community financial contributions. Not only does Rest for Resistance publish original writing like this by queer people of color – we are also working on a directory of mental health resources created by others living at the intersections of oppression. Donate to make those dreams a reality and put money towards the support of QTPoC.
Edited by O.A.O.
We need community support to continue publishing!
Articles and artwork like these are only possible through your contributions. Please donate today to sustain the wellbeing of artists, writers, healers, and LGBTQ2IA+ people of color.
You can also support our team by picking up
a Rest for Resistance print zine.
Image description:
A person wears a faux hat and black jacket, while staring down at a blue lip balm container whit one finger rubbing the inside. The person is standing in front of a closed establishment that has yellow gate covering the inside.
About Eli Sleepless:
Eli Sleepless is a self-taught latinx film photographer. Their genderqueerness and nyc upbringing is important to their work. Find more of their work on tumblr, instagram, facebook, and our main page.
About Dom Chatterjee:
The editor-in-chief of Rest for Resistance and founder of QTPoC Mental Health, Dom believes in the power of community to combat oppression. Dom is a non-binary desi-dutch-american person living with multiple disabilities.